Warning: Constant WP_CACHE already defined in /home/smbalnoi/backup.drsmbalaji.com/wp-config.php on line 86
Warning: The magic method Vc_Manager::__wakeup() must have public visibility in /home/smbalnoi/backup.drsmbalaji.com/wp-content/plugins/js_composer/include/classes/core/class-vc-manager.php on line 203 Surgery – Page 6 – Balaji Dental and Craniofacial Hospital, Chennai, India
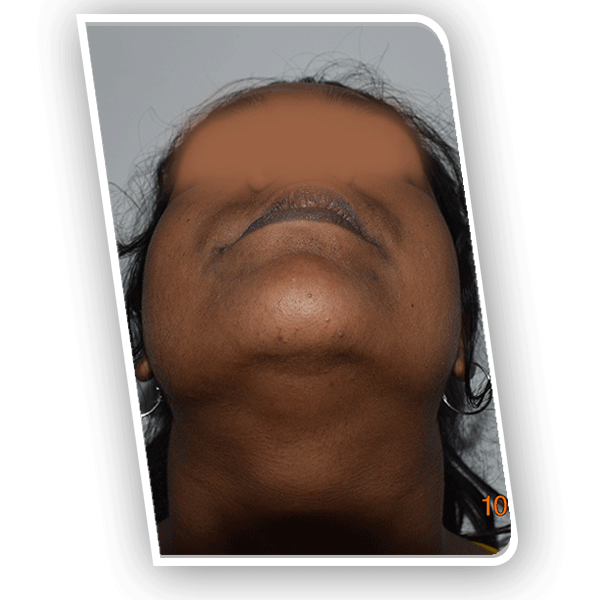
Patient develops a swelling in the region of the maxillary right anterior teeth
The patient is a 24-year-old female from Nanguneri in Tamil Nadu, India. Over a period of two years, she had begun to notice a slow growing swelling in the maxillary right incisor region. Since there had been no pain or discharge associated with it, she had ignored it for a long time. It was firm to the touch and not painful.
Some of her neighbors soon began commenting on the subtle change in her facial structure. It was only then that she decided to seek medical opinion for her upper jaw bone defect. Her parents had been referred to a nearby city hospital by some well wishers.
A biopsy had been obtained by the oral surgeon, which revealed a diagnosis of benign ossifying fibroma. He explained that this needed to be excised. Teeth in the involved region would be extracted. Artificial teeth would be placed once the surgical site had healed. The patient was particular that she did not want a removable denture.
What is a benign ossifying fibroma and what are its causes
This arises from the periodontal ligament and can be considered to be a benign neoplasm. There is expansion of the overlying cortical plates. Perforation of the overlying structures is never seen due to the slow growing nature of the lesion. Differential diagnosis includes reactive hyperplasia
Surgical excision of the benign ossifying fibroma from the maxillary bone
The patient underwent excision of the lesion along with extraction of the overlying right central and lateral incisors and the right canine. After a period to allow for complete healing of the surgical wound, the patient was referred to a prosthodontist. Rehabilitation was completed by constructing a bridge to replace the three extracted teeth.
The patient however was not happy with her postoperative appearance. She felt that her right alar base and lips had a sunken appearance. There was also food impaction in the region above the bridge, which was causing halitosis. The patient desired correction of her complaints.
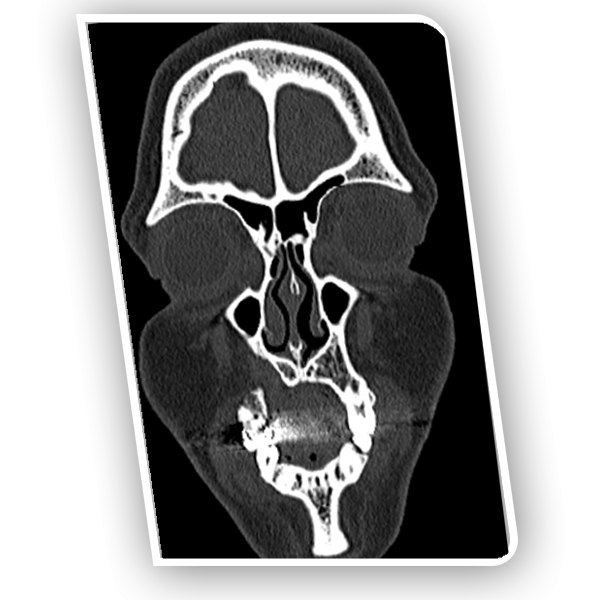
She therefore presented with a general surgeon who obtained imaging studies. Seeing that the bony defect was very large, he counseled her to approach an expert oral and maxillofacial surgeon. The patient made enquiries and was referred to our hospital for management.
Patient presents at our hospital for initial consultation for her bony defect
Dr SM Balaji, jaw reconstruction specialist, examined the patient and obtained imaging studies. This revealed that the patient had a defect of around 14 mm. He explained to the patient that rib grafts needed to be harvested for filling in the jaw defect. This would be followed by placement of dental implants to complete rehabilitation for the patient.
Successful reconstruction of the jaw defect using rib grafts harvested from the patient
Under general anesthesia, an inframammary incision was made and rib grafts were harvested. A Valsalva maneuver was then performed to ensure that there was no perforation into the chest cavity.
Attention was next turned to the region of the maxillary bony defect. A mucogingivoperiosteal flap was raised to expose the defect. The rib bone graft was then crafted to perfectly fit into the bony defect.
These were then fixed in place with titanium screws. Hemostasis was checked and the flap was closed with sutures.
Patient instructed to return in four months for dental implant surgery
Bony consolidation of the grafts to the surrounding alveolar bone would take up to four months. The patient was therefore instructed to return after four months for dental implant surgery. She expressed understanding of the instructions and thanked the surgical team before discharge from the hospital.
Patient with chronic tooth infections in his maxillary anterior teeth
The patient is a 28-year-old male from Pune in Maharashtra, India. He is an entrepreneur with his own startup company. Around 12 years ago, he had been injured while playing hockey in school. This had resulted in the fracture of his maxillary central incisors, left lateral incisor and left canine.
He had undergone root canal treatment of the four teeth along with bridge fixation. This had however turned into a chronic problem for the patient. He regularly developed pain and swelling in the region. This had been a constant source of discomfort for the patient.
Multiple apicoectomy procedures had been performed over the years for the involved teeth. This had however not provided long term resolution of his symptoms. His teeth had also become mobile due to bone loss from recurrent infections to the area.
Social difficulties arising from his long standing dental problem
The patient has also had long standing problems with food impaction and resultant halitosis. This had gotten to the point that it began affecting his work. He then decided to seek a permanent solution to this long standing problem.
The patient had visited a dental clinic where imaging studies had been obtained. The dental professional had also conducted a thorough intraoral examination.
This had revealed highly mobile teeth along with extensive alveolar bone loss and gum disease. Periodontal ligament attachment had been destroyed. There was also a periapical cyst in relation to the affected region.
The patient was informed that he needed treatment from an experienced oral and maxillofacial surgeon for his problems. He was then referred to our hospital for treatment. Oral and maxillofacial surgery in a cutting edge superspecialty at our hospital.
The patient had subsequently researched our hospital over the Internet. He made further enquiries using his professional contacts in Chennai. Having finally satisfied himself about the quality of services, he had contacted our hospital manager and made an appointment.
Initial consultation at our hospital to address his long standing dental difficulties
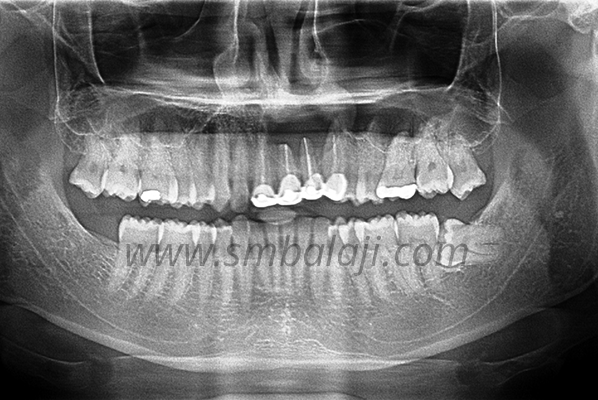
Dr SM Balaji, bone graft dental implant specialist, examined the patient and obtained imaging studies. This revealed that the patient had root canal treated upper central incisors and left lateral incisor and canine. There was extensive alveolar bone resorption of the involved area. This had resulted in grade 2 anterior mobility of the involved teeth.
It was explained to the patient that it was just a matter of time before the teeth were lost. He was advised upper jaw reconstruction with bone grafts. This would be followed by fixing of implants to the rib grafts. Final step of rehabilitation would involve fabrication of a bridge to replace the missing anterior teeth.
This was explained to the patient in detail and he consented to undergo surgery.
Successful placement of rib grafts along with dental implants in the maxillary anterior region
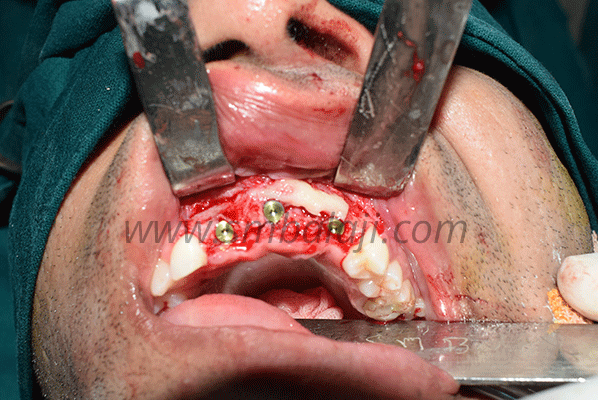
Under general anesthesia, a mucogingivoperiosteal flap was first raised over the region of the involved teeth. The four involved teeth were extracted and the cystic lesion was removed in its entirety. Friable infected bony tissue was then removed with a bur.
Attention was then turned to harvesting the bone graft. An inframammary incision was made followed by harvesting of a rib graft. This was followed by a Valsalva maneuver to ensure that there was no perforation into the thoracic cavity. The incision was then closed in layers with sutures.
The bone graft was then crafted to fit perfectly into the region of bony defect in the anterior maxillary region. This was then fixed in position with titanium screws. The patient was instructed to return in four months for fixation of implants in the bone grafts.
It would take a period of four months for complete bony consolidation of the grafts with the surrounding alveolar bone.
Patient returns in four months for placement of dental implants
The patient returned after a period of four months for dental implant surgery.Three Nobel Biocare dental implants were fixed in the consolidated bone grafts. The patient was instructed to return after four months for placement of a dental bridge.
He reported back as instructed after osseointegration of the implants to the alveolar bone. A Ceramic bridge was then fabricated to complete the rehabilitation process for the patient.
The patient was very satisfied with the results of his treatment. He said that he could not even differentiate between his natural teeth and the ceramic bridge. The patient thanked the entire team before final discharge from the hospital.
Patient born with a cleft lip, palate and alveolus to closely related parents
The patient is a 3-month-old baby from Pathankot in Punjab, India. She was born with a right-sided cleft lip, palate and alveolus. Of note, there is a family history of an uncle with a cleft lip, palate and alveolus deformity. Her father’s younger brother was born with the same deformity on the left side.
Mother had undergone routine prenatal care including an ultrasound of the fetus. This revealed the cleft deformity in the growing fetus. The parents were however unfazed by this development. Her uncle had undergone surgical correction of his facial deformities at our hospital nearly two decades ago.
Total rehabilitation of her uncle for his cleft deformities at our hospital
He had undergone cleft lip repair at 3 months and cleft palate repair at 8 months. His speech difficulties had been corrected by a pharyngoplasty at 3-1/2 years of age. As his cleft alveolus deformity had been significant, he had undergone bone grafting at 5 years of age.
He had hardly noticeable scarring from the surgeries and had never faced any difficulties secondary to his deformities. Always an excellent student, he is now pursuing his undergraduate studies in medicine. His ambition is to become a facial plastic surgeon dealing with congenital deformities of the face.
Parents had got in touch with our hospital soon after the ultrasound diagnosis for their child. Dr SM Balaji studied the ultrasound images in detail. He then advised them to come to the hospital when the child was 3 months old.
International accolades for the cleft surgical correction services of our hospital
Cleft repairs are routinely performed in our hospital. Facial plastic surgery is also a specialty offering at our hospital. Scores of patients have been rehabilitated with the optimum cosmetic outcomes. Nasal mucosal reconstruction and soft palate repair is also a component of cleft palate repair.
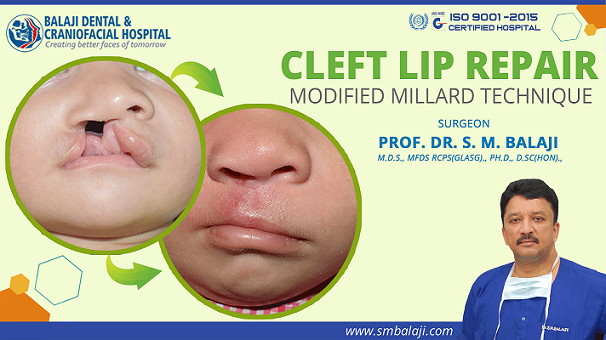
Before Surgery
After Surgery
Initial presentation at our hospital for consultation of her cleft deformity correction
Parents presented at our hospital when the child had attained 3 months of age. Her uncle too accompanied them. He was very familiar with all the members of the surgical team and greeted them. Everybody expressed their happiness at the great strides he was making towards attaining his ambition.
Dr SM Balaji, cleft lip and palate surgeon, examined the child. She had a buckled columella from the cleft deformity. There was also a split upper lip from the right-sided cleft lip defect. She also had a widened alar base defect to the nose.
Dr SM Balaji counseled the parents extensively. He said that the cleft lip surgery would be followed by cleft palate surgery at 8-10 months of age. Explaining further, he said that rh-BMP might be required for the cleft alveolus if the defect was large.
Pharyngoplasty might also be required if the patient develops any speech problems. Meticulous treatment planning was performed for the patient. It was decided to perform a modified Millard’s cleft lip repair for the patient. Her parents expressed complete confidence with the treatment plan and consented to surgery.
Successful surgical correction of right-sided cleft lip and nasal floor deformity
Under general anesthesia, surgery was first begun with an incision along the philtrum with dissection down to the subcutaneous tissues. The nasal floor defect was addressed first. The nasal floor was reconstructed using the flap.
The nasal sill was then reconstructed using a C-flap. A three layer lip closure was utilized as it offered the best cosmetic and functional results for the patient. The skin, subcutaneous connective tissue and muscles were reapproximated and joined with great precision. This resulted in optimal reconstruction of the lip vermillion border, philtrum and orbicularis oris muscle.
Nasal floor was reconstructed by raising the alar base. This gave good symmetry to the nasal correction. Fine 4-0 Vicryl sutures were used to close the incision in layers for minimal scar formation. The entire surgical procedure was performed under magnification through utilization of a surgical loupe.
Optimal postoperative results by the seventh postoperative day
The patient was gurgling and cooing by the seventh postoperative day. Scarring was minimal and would reduce further with the passage of time. The proud parents and uncle were extremely happy with the results of the operation. Patient had a good suckling reflex and had gained nearly 1 kg within the few days following surgery.
Further instructions given to the parents and uncle regarding patient
It was further reiterated to them that the road to complete rehabilitation was a long one for the patient. They expressed their complete confidence in the surgical team, which was essentially unchanged from the one that had treated the uncle. Expressing their thankfulness to everyone, they said that they will return in a few months for the cleft palate repair.
The patient has a freak accident at home while relaxing on a weekend
The patient is a 22-year-old male from Chennai in Tamil Nadu, India. He was relaxing at home on a weekend after completing his examinations. Walking into the balcony of his house in the dark, he had tripped on his dog. The fall had resulted in a direct impact to his midfacial region from a cushioned wooden swing.
He had felt an excruciating pain immediately upon impact and had cried out loudly. Hearing his cry, his parents had rushed to him. There was bleeding from inside his mouth and he appeared dazed from the impact.
They rushed him immediately to a nearby dental clinic. An intraoral examination had revealed a mobile maxillary bone along with a laceration near the maxillary labial frenum.
He had been diagnosed with a maxillary fracture and the laceration had been sutured. Once bleeding had been stopped, he had been referred to our hospital for management of his fracture. Our hospital is a leading center for facial fracture surgery in India. Jaw fracture surgery for complicated maxillary and mandibular fractures are routinely performed in our hospital
Patient brought to our hospital for management of his maxillary fracture
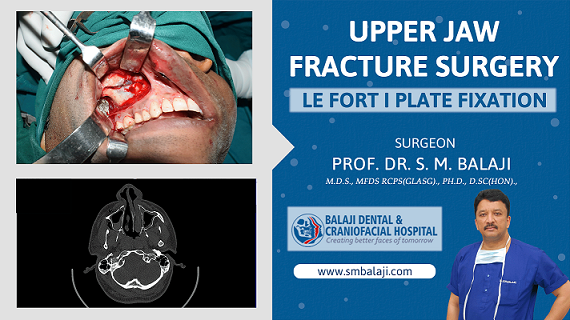
Dr SM Balaji, jaw fracture specialist, examined the patient and ordered imaging studies including a 3D CT scan. Examination revealed that the entire maxillary segment was mobile. There was the complete horizontal separation of the maxilla from the skull. Horizontal maxillary fractures are also known as the floating palate.
There was no involvement of the orbital wall or the inferior orbital rim. The Zygomatic arches were also intact. There was no other facial injury other than the broken jaw and labial laceration. Oral surgeons in India are the primary surgeons for this injury.
All relevant testing was performed on the patient. There was no loss of sensation or abnormal sensations present in the region of the fracture. There was no ecchymosis to the skin overlying the fracture. The patient and his parents were informed that he had a maxillary Le Fort I fracture.
Treatment planning was explained to the patient and his parents in detail. All their fears and doubts were allayed. They were reassured that the patient would make a complete recovery from the fracture. The patient and his parents then consented to surgery.
Successful surgical reduction of the horizontally fractured maxillary segment
Under general anesthesia, the maxilla was examined and demonstrated crepitus with movement. A right maxillary lateral vestibular incision was made. Dissection was made down to the region of the fracture.
The fracture segments were stabilized and occlusion was checked. This was then fixed with two four-holed L-shaped titanium plates and screws.
Attention was next turned to the left side where two four-holed straight titanium plates were used to stabilize the fracture. Occlusion was checked again and found to be intact. All incisions were then closed with sutures. The patient was then extubated and taken to recovery in stable condition.
Complete restoration of esthetics and function following maxillary fracture reduction surgery
The patient made a full recovery and returned to normal life. He said that there was no change in his facial appearance and no pain. His parents were extremely relieved that he had made a complete recovery from his jaw fracture. They expressed their thankfulness to the surgical team for their son’s recovery.
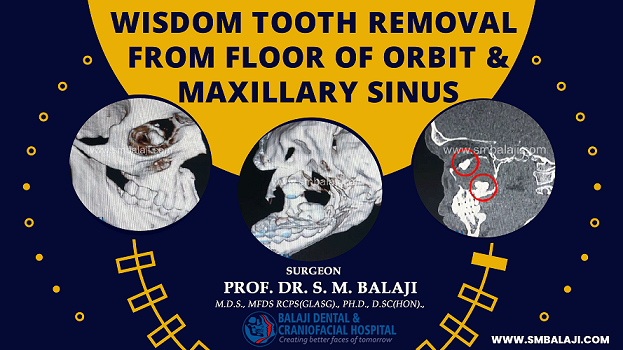
Wisdom Tooth Removal from Floor of Orbit and Maxillary Sinus
Patient with a long-standing history of midfacial stuffiness and dull pain
The patient is a 22-year-old male from Chennai in Tamil Nadu, India. He began feeling a heaviness in the maxillary region about a year ago. The tone of his voice also felt muffled. He said that he developed a throbbing feeling in his right midface region.
There was also a persistent dull headache that was present most of the time. He also had a discharge from his nose that had a foul smell.
The patient underwent a course of antibiotics and antihistamines that were prescribed at a local hospital. However, this offered no relief from his symptoms. The doctor has then obtained imaging studies that showed the presence of a tooth in the floor of his right maxillary sinus.
It was felt that the patient needed a dentist or oral surgeon to address his problem. He had then been referred to our hospital for surgical management of his impacted tooth.
Initial consultation at our hospital for management of his impacted tooth
Dr SM Balaji, maxillary sinus impaction specialist, examined the patient and obtained imaging studies including a 3D CT scan. This showed an additional finding of an impacted tooth in the floor of the right orbit. There was also the previously diagnosed impacted tooth on the floor of the maxillary sinus.
A biopsy of the lesion returned with the diagnosis of maxillary sinus dentigerous cyst. The cyst lining had proliferated to fill up the entire sinus cavity. Air is normally present within the paranasal sinuses to provide resonance to the voice.
Maxillary dentigerous cysts are relatively uncommon when compared to mandibular dentigerous cysts. However, treatment remains the same with complete enucleation of the cystic lesion from the surrounding bone.
Treatment planning was explained to the patient in detail. He expressed understanding of the treatment plan and consented to surgery.
Successful surgical removal of impacted molars from orbital and sinus floor
Under general anesthesia, a gingivoperiosteal flap was raised in the right posterior maxillary (gum tissue) region. Access was gained into the maxillary antrum. Exploration of the sinus cavity was done. The impacted wisdom tooth was identified.
There was a dense proliferation of the cystic lining, which completely filled the antrum. This was the reason behind the feeling of fullness and heaviness that he had complained about.
The infected dentigerous cyst lining was removed from the antral cavity. Care was taken to ensure that no remnant of the lining was left behind in the maxillary antrum. The impacted molar in the floor of the mouth was then extracted. This was followed by extraction of the impacted tooth on the floor of the orbit.
Thorough irrigation with saline solution was then performed. Extreme care was taken to ensure that there was no damage to any of the surrounding tissues. The gingivoperiosteal flap was then closed with sutures. General anesthesia was reversed and the patient was taken to the recovery room.
Complete satisfaction from the results of the surgery with a resolution of symptoms
The patient stated that his head felt good for the first time in many years. He said that the midfacial heaviness and stuffiness had completely resolved. His voice also sounded more resonant and the dullness to it was completely absent.
He also said that his breathing also felt better and the air felt fresh and more invigorating. The patient and his family thanked the surgical team before the final discharge from the hospital.
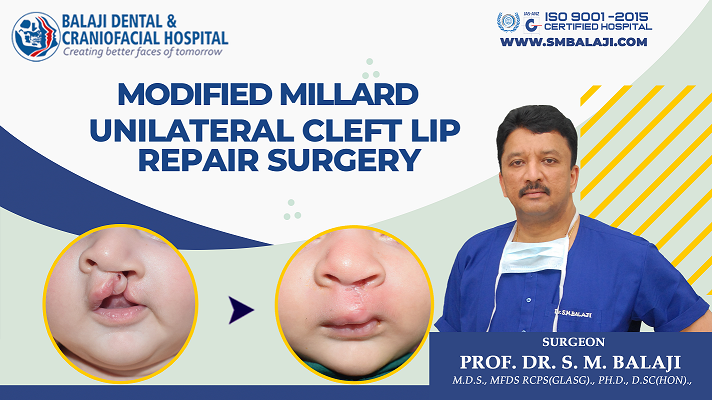
Patient born with a unilateral cleft lip, palate and alveolus deformity
The patient is a 3-month-old female infant from Ajmer in Rajasthan, India. She was born with a left-sided cleft lip, palate and alveolus deformity. Her upper lip was split because of the cleft lip.
There was a communication between the oral and nasal cavities through the roof of the mouth. This had devastated the parents. Cleft defects are the most common form of birth defects affecting newborns.
Hospital staff had provided extensive counseling for the family and educated them about the condition. Parents were most distressed by her feeding difficulties. Friends had informed them that they needed to approach a facial plastic surgeon.
Contact with parents of another child who had undergone cleft deformity repair previously
The hospital had referred the parents to the parents of another child who had been born with cleft deformity a few years ago. Parents immediately got in touch with them. They also met the child who had been born with a cleft defect. The child was now 6 years old and appeared normal with completely normal speech.
The parents were informed that Dr SM Balaji had operated on their daughter. They also informed that this surgery had been a little over five years ago. All their fears regarding the deformity affecting their child had been allayed over the years following cleft surgery. They said that their daughter had not faced any problems because of her cleft defect.
Parents immediately obtained contact information about our hospital and got in touch with our hospital manager. They had then been given an appointment to meet Dr SM Balaji for a consultation.
Center of excellence for cleft lip repair in the entire Southeast Asian region
Our hospital is a premier cleft lip surgery hospital in India. We are recognized as a center of excellence for cleft lip surgery by the International Cleft Lip and Palate Foundation (ICPF) of Japan.
We are the proud recipients of the prestigious ‘Prof David Precious Award.’ This was awarded in recognition of innovations developed by us for the rehabilitation of cleft patients. We are also an affiliate of the Dallas-based World Craniofacial Foundation (WCF).
Before Surgery
After Surgery
Initial presentation at our hospital for rehabilitation of her cleft lip defect
Dr SM Balaji, cleft repair surgeon, examined the patient. The patient had buckling of the columellar cartilage. There was a widened alar base defect and the floor of the nose was nonexistent.
The nasal sill was also absent on the left side. There was also a cleft alveolus defect. It was explained to them that modern surgical intervention would leave minimal discernable scars depending upon the skin condition.
They were reassured that the patient would lead a completely normal life. The surgical schedule was explained to them in detail. Importance of adhering to the timetable was explained to them.
Correct time schedule for performing each step of cleft deformity repair
They were informed that cleft lip surgery needed to be done at 3 months of age. This would be followed by cleft palate surgery at 8-10 months of age. Cleft alveolus repair may be needed between 4-5 years of age. This will be performed with rh-BMP if there is a large alveolar defect.
Pharyngoplasty may also be required if the patient develops speech problems. Speech therapy would also be needed in case of issues with speech.
Meticulous treatment planning was performed for the patient. Thorough biometric studies were ordered and a projection of growth was predicted for the reconstruction and surrounding structures.
A modified Millard’s cleft lip surgery would be performed for repair of the patient’s cleft lip. This planning protocol would ensure the best possible symmetric and functional repair for the patient. Parents expressed understanding and consented to surgery.
Successful repair and reconstruction of unilateral lip and nasal deformities
Under general anesthesia, an incision was made along the philtrum and dissected down to the subcutaneous tissues. Attention was first turned to the nasal floor defect. This was then reconstructed.
A C-flap was raised for recreation of the nasal sill. A surgical loupe was used to visualize the surgical site during the entire procedure.
It was decided to utilize a three-layer closure of skin, subcutaneous tissue and muscle to obtain the best possible esthetic results. There was good recreation of the vermillion, philtral column and orbicularis oris. Nasal floor recreation resulted in raising of the alar base. Fine 4-0 Vicryl sutures were utilized for closure of the cleft defect.
Successful postoperative healing of cleft defect with optimal results
By the seventh day following surgery, there was just minimal scarring at the site of the surgical repair. The patient had developed a good suckling reflex following surgery and began to feed well, gaining weight. Establishment of symmetry of the lips results in pleasing facial esthetics. Parents were very happy with the results.
It was explained to the parents that this was just the first step in the long road to rehabilitation for the patient. They expressed complete understanding of this and were committed to sticking to the surgical schedule that had been provided to them.